















 817 860
817 860

subfascial catheters are placed to infuse a constant rate of local
anesthetic.
2.3.
Postoperative course
Post-operatively, patients are admitted to a non-monitored bed and
started on sips of clear liquid immediately. When an epidural is present,
we emphasize non-narcotic medication infusion. We routinely use
ketorolac and acetaminophen, with narcotics reserved for breakthrough
pain. A regular diet is resumed on postoperative day 1, regardless of
return of bowel function, defined as flatus or bowel movement. The
epidural, if present, is typically removed on postoperative day 2. Patients
are discharged once routine criteria had been met.
2.4.
Postoperative follow-up
Post-operatively, patients return for clinic follow-up within 1–2 wk.
Surveillance protocols follow the 2014 National Comprehensive Cancer
Network guidelines
[5] .2.5.
Data analysis
Two independent reviewers retrospectively reviewed outcomes. Com-
plications were graded according to the Clavien-Dindo classification. A
descriptive analysis using SAS was performed. Ileus was defined as no
flatus or bowel movement for longer than 4 d postoperatively.
3.
Results
One patient required conversion to a TP approach for failure
to progress, leaving 68 patients who underwent an EP
approach successfully. The median age of the cohort was
28 yr (range 17–55). The median follow up was 15.3 mo
(interquartile range [IQR] 5.7–24.3 mo). Of the 68 patients in
the cohort, 27 underwent primary RPLND and 41 underwent
PC RPLND. In the PC group, 37 patients had nonseminoma-
tous GCT, while four had seminomatous disease.
According to axial measurements of preoperative
images, six patients (8.9%) had no retroperitoneal involve-
ment, 23 patients (33.8%) had a retroperitoneal mass of
<
2 cm, 15 (22.1%) had a mass of 2–5 cm, and 24 had a mass
of
>
5 cm, of which 19 (27.9%) were
>
10 cm
( Table 1 ). Three
patients underwent cavectomy at the time of RPLND. The
median overall mass size on preoperative imaging was
2.2 cm (IQR 1.3–5.1).
Intraoperative outcomes were as follows. Median
estimated blood loss (EBL) was 325 ml (IQR 200–612.5)
and the median number of units of packed red blood cells
transfused was zero (range 0–7). The median total number
of nodes resected was 36 (IQR 24.5–49); the median
number of positive nodes was 1 (IQR 0–4).
Postoperatively, the median time to return of bowel
function, defined as either flatus or bowel movement, was
postoperative day 2 (range 2–4 d). There were no cases of
ileus. The median LOS was 3 d (range 2–4 d).
Eleven patients had 12 (17.6%) complications at 90 d, of
which six (55%) were Clavien grade 1 and five (45%) were
grade 2
( Table 2 ). There was one grade 3 complication
(1.5%), which was a chylous fluid collection requiring
imaging-guided drain placement (grade 3b); the drain was
removed in the clinic 2 d later. In the primary group,
prospective nerve-sparing was performed in all patients.
Two patients did develop retrograde ejaculation; one had
stage IIA seminoma upstaged to stage IIB at the time of
RPLND, and the other has primary stage IIA NSGCT. Nerve
sparing could be performed in 32 of the PC cases, with an
antegrade ejaculatory rate of 96.8%
( Table 3).
The most common complication category was infection.
Four patients (5.9%) had symptomatic anemia postopera-
tively that required transfusion. There was one readmission
for nausea with vomiting on postoperative day 23, which
resolved with intravenous fluids and antiemetics.
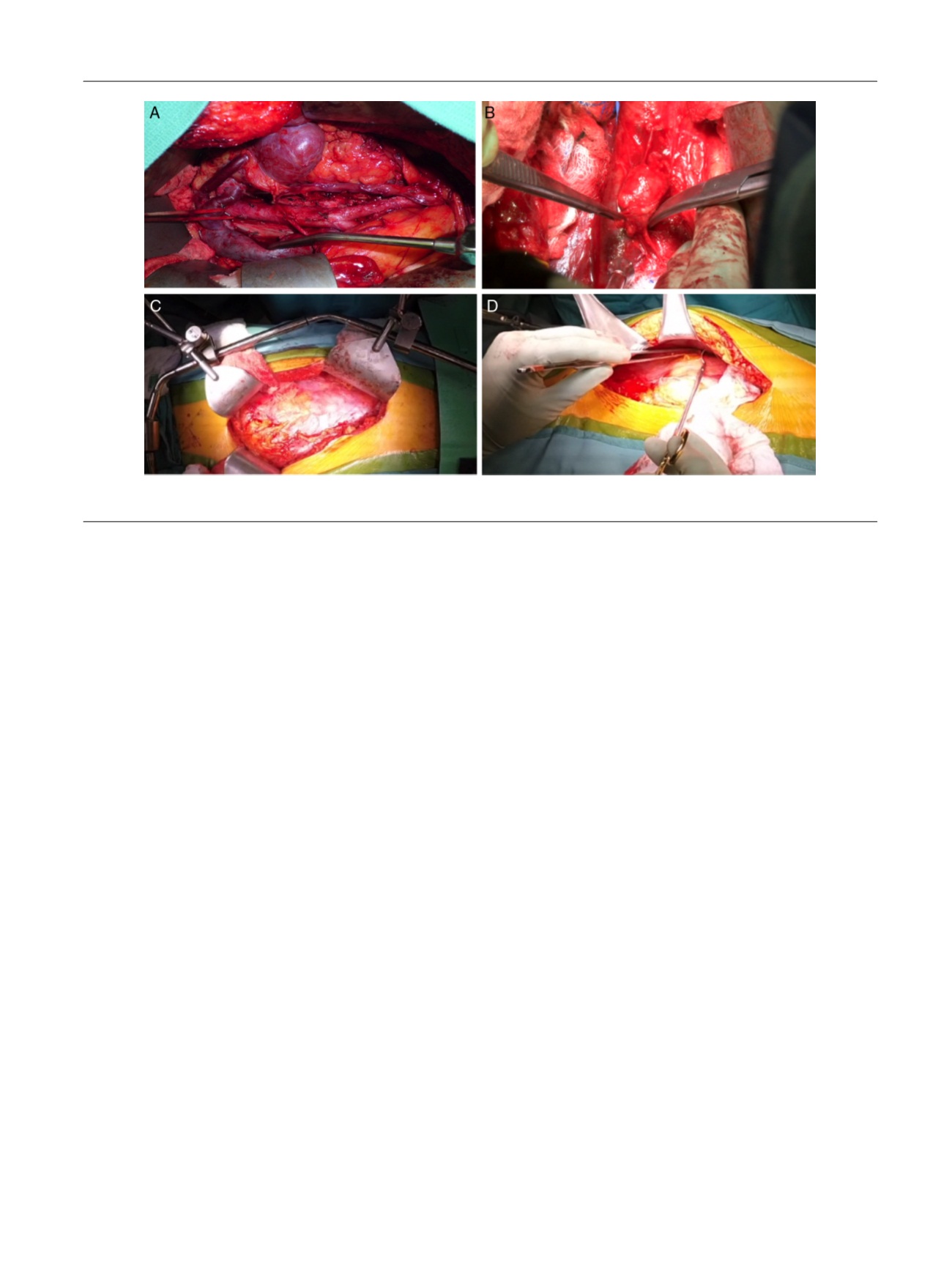
[(Fig._3)TD$FIG]
Fig. 3 – (A) Left-sided full bilateral template. (B) Lymph node dissection. (C) Release of the peritoneal sac. (D) Closure of the peritoneotomies.
E U R O P E A N U R O L O G Y 7 2 ( 2 0 1 7 ) 8 1 4 – 8 2 0
817